Live Event
Real solutions from experts who've moved the needle on burnout
Register Now![]() Features
Features
TABLE OF CONTENTS

It’s that time of year! Spring has (mostly) sprung, and Opening Day has officially arrived for Major League Baseball.
To give you an idea of scope, the 2022 MLB season featured more than 1,200 players, 2,400 games, and 64 million fans crowding into stadiums. And here’s something that’ll blow your mind: Over the course of just 10 seasons, it’s actually possible to generate more MLB schedule options than there are atoms in the universe. Yes—you read that right.
But even taking that staggering fact into account, you may be surprised to learn that a season of baseball scheduling is still much less complicated than just one month of scheduling for around-the-clock shifts in a hospital ED. Anyone who’s been in charge of putting that schedule together will tell you it’s a stressful process. If it’s done with paper and spreadsheets, it’s an exercise in madness.
Believe it or not, the responsibility of scheduling MLB games used to fall on the shoulders of a man in the commissioner’s office named Harry Simmons. Over time, the task of scheduling became so onerous that it turned into Harry’s full-time job. That progression probably sounds familiar to some of our readers!
In the early 1980s, the league transitioned scheduling duties to a husband-and-wife duo named Henry and Holly Stephenson. They built schedules for 20+ years using a mix of computers and manual handiwork. During this time, enterprising folks at IBM, MIT, Stanford, and Carnegie Mellon tried repeatedly to unseat the Stephensons from their role with computers. This didn’t work until 2005, when the league finally started generating schedules using technology called combinatorial optimization.
MLB’s tech-enabled scheduling process has incorporated even more nuance in the years since it was adopted. For the 2023 season, a more evenly balanced schedule was the top priority. The new format allows teams to play a greater percentage of games against non-divisional opponents, meaning schedule difficulty from team to team will have far less variance. The lesson? Balanced schedules are a win for everyone. Imagine that!
This combinatorial optimization technology has spread to all sports leagues, as well as other applications like airline schedules and retail stores. Any time you’ve got a mix of variable factors—teams, people, holidays, facilities, weather patterns, fluctuating demand—and lots of rules that could be ripped from a high school word problem, you need advanced computing to make a proper schedule out of it.
But despite the proliferation of this technology elsewhere, healthcare is still behind the curve. Somewhere out there tonight, a tired neonatologist (for example) is spending hours—and maybe multiple days—poring over spreadsheets and texting colleagues from her group to gather all the information she needs to put the schedule together for the next month. This is a common occurrence, and it’s a problem that can’t be ignored any longer. Manual scheduling takes far too much time, it carries the risk of human error, and it can be a major contributor to burnout.
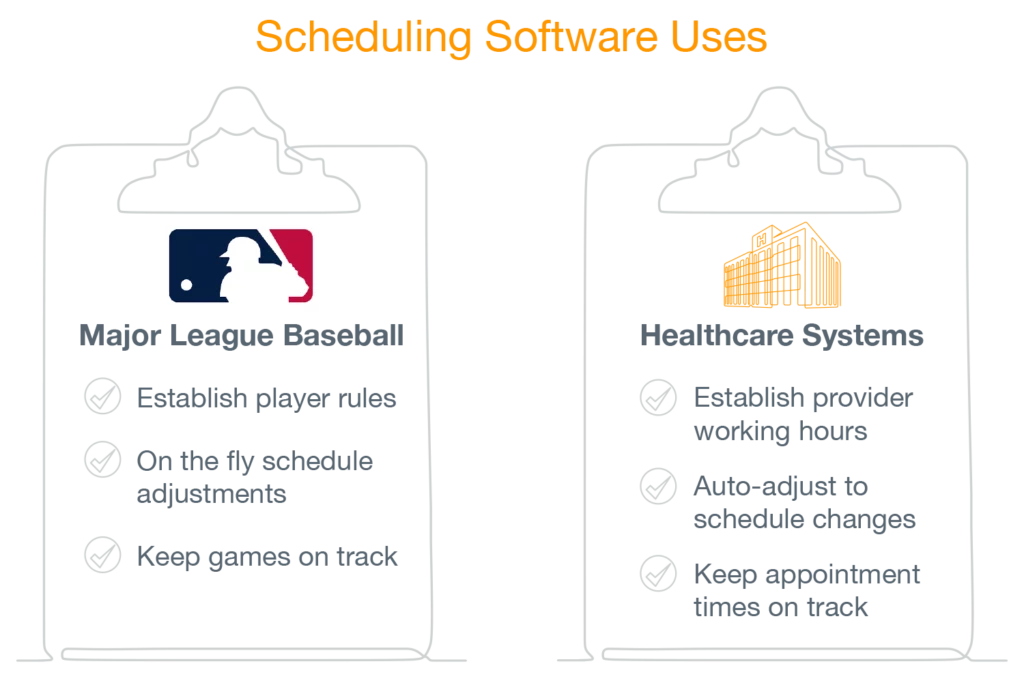
The MLB has two ways of using scheduling software:
As it turns out, healthcare uses scheduling software much the same way:
A Lightning Bolt study of more than 5,500 real medical department physician shift schedules revealed that schedule complexity varies by specialty. With an average of 62 repeating scheduling rules and 276 monthly schedule change requests, emergency medicine has far and away the most complex process. Hospital medicine and OB-GYN are next, while office-based schedules like nephrology are simpler but still more complex than what you’ll find in the MLB. The number of schedules that can be generated with the complexity and variability inherent to emergency medicine is hard to fathom. Interestingly, a recent report from Medscape revealed that 65 percent of emergency medicine physicians reported burnout—the highest rate of any specialty.
It’s time for more healthcare leaders to understand what the MLB has known since 1981: when it comes to building complex schedules, technology is your best bet. Using machine learning to balance dozens of rules and to support flexibility for ongoing changes is good practice for baseball players, pilots, and physicians alike.
So when it comes to aiding physician retention and preventing staff burnout with better scheduling technology, isn’t it time for the healthcare industry to play ball?